Unicondylar Knee Replacement in Early Osteoarthritis Knee – an alternative to Total Knee Replacement
Osteoarthritis (OA) of the knee is a major clinical burden with over 25% of people aged over 55
years suffering knee pain on most days of the month. Management of OA involves a step-wise
approach based on the severity of symptoms, beginning with preventive approaches involving
alignment correction and cartilage regenerative procedures as well as pharmacological pain
controlling strategies, and finally, joint resurfacing and arthroplasty to be considered for advanced
stages of disease.
The primary indication for Knee Arthroplasty is significant and disabling pain due to severe OA.
Depending on the location and severity of OA within the knee joint, several options may be
considered, including Total (TKA) or Partial Knee Arthroplasty (PKA).
While the conventional approach to total knee replacement uses implants to reconstruct all the
compartments of the knee, a total knee replacement may not be necessary for all patients. In knees
that are otherwise healthy with involvement of single compartment, a partial knee replacement can
preserve the healthy bone, cartilage and ligaments. Partial knee replacement may be either involve
Patello-Femoral Joint Arthroplasty or Unicompartmental Arthroplasty.
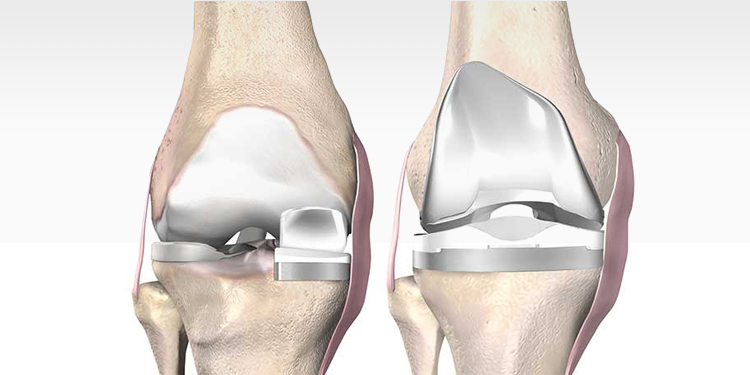
Unicompartmental, or unicondylar, knee arthroplasty (UKA)
Unicompartmental, or unicondylar, knee arthroplasty (UKA) is the preferred procedure when the
aim is to preserve the intrinsic joint stabilising structures, as well as healthy joint compartments.
Here, the partial knee implant is designed to repair only the damaged portion of the knee joint, i.e.,
either the medial or lateral condyle. Thus, it makes the implant much smaller than a conventional
total knee implant.
Evolution of UKA
UKA was introduced in 1970s with the promise of minimal bone loss and the potential ease of
future revision to a TKA if required. However, an inadequate understanding of appropriate
indications and surgical techniques, combined with suboptimal early prosthetic designs resulted in
an unacceptably high rate of failure early on and made the surgery quite unpopular at the time. But
advancements in UKA implant designs and improved surgical techniques in recent years have lead
to renewed interest in UKA . The resurgence of this less invasive knee arthroplasty is also
secondary to reports of excellent survivorship rivalling TKA in appropriately selected patients.
conventional total knee implant.
Indications for UKA
Careful selection of patients is the key to a successful UKA. Current indications for UKA
implantation are: isolated unicondylar osteoarthritis (OA) or osteonecrosis (identified radiologically
as bone-on-bone arthritis); frontal deformity < 15°; flexion contracture < 15°; functional integrity of
the anterior cruciate ligament (ACL) and peripheral ligaments of the knee, as well as the absence of
any inflammatory arthropathy. Indians are potential candidates for UKA because of our genetic
predisposition for tibia vara and antero-medial OA.
Advantages
UKA with microplasty instrumentation is definitely the ‘game changer’ in Knee Arthroplasty. This
less invasive surgery involves a smaller incision, removes less tissue, and preserves upto 80% of the
normal bone. Blood transfusions are generally not needed and this surgery is least associated with
intra-operative complications, infections, venous thromboembolism, cardiovascular events, etc.
Patients experience less pain and recover faster and the hospital stay is shorter compared to TKA.
Patients can walk on their surgical leg on the same day as the surgery. Since the knee ligaments are
preserved, near-normal kinematics is restored and patient gets the feeling of a ‘natural’ joint. Return
to low-to-intermediate sports within 3-6 months of the surgery is also possible without any
problems.
Disadvantages
Unicondylar knee replacement surgery can be extremely successful but most surgeons agree that it
is a more technically demanding procedure relative to TKA. Studies involving various National
Registries show a 3-times higher failure/revision rate for UKA compared to TKA making even
competent surgeons hesitate. 90% complications are due to the tibial side failure (overload). Tibial
strain increases by 60% following UKA causing antero-medial tibial pain following surgery. But it
has been found that the increased strain occurs with surgical errors like deep vertical cut, medial
vertical cut and deep tibial resection.
There are virtually no contraindications for UKA, but it must be avoided in patients with
inflammatory arthritis and morbid obesity.
Conflict between TKA and UKA
The dilemma faced by Orthopaedic surgeons across the world is whether to do a TKA or UKA for
isolated unicondylar osteoarthritis. The fear of early revision seems to have reduced the prospects of
UKA but what surgeons need to identify is that higher revision rates are mostly because of
subjective surgeon reasons; it is therefore more important to master the technique rather than to
repudiate the procedure altogether. Further, even TKAs fails. Though, the incidence of failure after
knee replacement is low, it has been reported that more than 22,000 knee replacements are revised
yearly for aseptic loosening, instability, infection, etc.
In decisions about which procedure to offer, the seemingly higher revision/re-operation rate of UKA
than of TKA should be balanced against a lower occurrence of complications, readmission, and
mortality, together with known benefits for UKA in terms of postoperative function. Conventional
UKA can be an economically attractive alternative in patients sixty-five years of age or older, and
modest improvements in implant survivorship could make it a cost-effective alternative in younger
patients.
Recent Advances
The difficulty with UKAs historically are the problems and failures from inaccurate placement.
Computer Navigation (CN), Robotic-Arm assisted (RA) UKAs are recent advances introduced to
increase accuracy and consistency of component placement. Pre-op CT based 3D anatomic
placement- 3D reconstruction of patients knee and patient specific anatomic planning assists
surgeons with optimal implant position and alignment. Robotic system allows to define alignment/
extension gaps/kinematics, consistent tracking and congruency through Range Of Motion, thereby
avoiding over/under correction. Robotic-assisted UKAs have demonstrated satisfactory clinical
outcomes, fewer revision and excellent survivorship on long term follow-up. However, as of now,
RA UKAs are associated with a longer operating time and increased cost to the patients. This
scenario may be improved by training new surgeons and by increasing the number of partial knee
surgeries at the given institution.
Summary
Partial knee replacement has many advantage over TKA. Understanding the indication is the key to
success of this minimal invasive surgery. Main indication is Antero-Medial Osteo Arthritis (boneon-bone OA) with intact ACL. However, broad indications have not been found to compromise
results. Improvements in implant design and surgical techniques of unicondylar knee arthroplasty
like Computer Navigation, and Robotics have led to reduced revision rates, but patient selection is
the most crucial factor for success of such arthroplasties.